Children with asthma: research Canadian Health Care Mall

In this article Canadian Health Care Mall will look at the problem of childhood asthma.
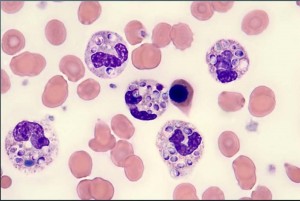
This case series is obviously limited by sample bias, and small sample size precluding simple generalizations. In addition, we cannot comment on whether our subjects had elevated numbers of mast cells within their airways, as Giemsa staining was not performed. With that said, mast cells were not found to be elevated in the study by Wenzel who found no difference between the number of mast cells within the airways of severe asthmatics compared to mild asthmatics and control subjects. Children with asthma referred to NJMRC often are among the most severe. In addition, only a minority of the children referred to NJMRC undergo bronchoscopy with biopsy.
Read more on Children with asthma: research Canadian Health Care Mall…
 Histoplasma capsulatum infection demonstrates a broad spectrum of acute and chronic clinical manifestations. Unlike the acute reaction to proliferating organisms, the chronic complications are often the result of excessive or prolonged host response with a paucity of organisms. Lung nodules (histoplasmomas) may be noted decades after initial infection and present a challenging clinical problem, as they can be difficult to distinguish from malignancy or tuberculomas. Typically, histoplasmomas are small (< 1 cm), asymptomatic, and may be stable in size or slowly enlarge over time. Here we report three patients with unusually large, or giant, histoplasmomas (> 3 cm) and describe their extreme phenotype. Importantly, two of the patients presented with subacute symptomatic disease, a presentation that is very atypical for histoplasmoma. The term “buckshot” calcification has been used to describe dozens of small (2-4 mm) calcified nodules, so it may be appropriate to label masses that exceed 3 cm as “cannonball” histoplasmoma.
Histoplasma capsulatum infection demonstrates a broad spectrum of acute and chronic clinical manifestations. Unlike the acute reaction to proliferating organisms, the chronic complications are often the result of excessive or prolonged host response with a paucity of organisms. Lung nodules (histoplasmomas) may be noted decades after initial infection and present a challenging clinical problem, as they can be difficult to distinguish from malignancy or tuberculomas. Typically, histoplasmomas are small (< 1 cm), asymptomatic, and may be stable in size or slowly enlarge over time. Here we report three patients with unusually large, or giant, histoplasmomas (> 3 cm) and describe their extreme phenotype. Importantly, two of the patients presented with subacute symptomatic disease, a presentation that is very atypical for histoplasmoma. The term “buckshot” calcification has been used to describe dozens of small (2-4 mm) calcified nodules, so it may be appropriate to label masses that exceed 3 cm as “cannonball” histoplasmoma. An exercise test was performed on a bicycle ergometer while subjects were breathing dry medical air in order to assess the presence of EIB, as well as the VL (see below). The power output was increased during the first 4 min in order to reach a target ventilation output that was > 60% of the predicted maximum voluntary ventilation (35 X FEV1) according to standard recom-mendations. To ensure that the ventilatory stimulus for EIB was sufficient, the exercise duration was modified compared with recommendations to a total of 16 min (ie, 12 min at target ventilation). In addition, increased exercise duration may lead to bronchoconstriction during exercise itself, and we hypothesized that this bronchoconstriction may promote VL. Spirometry was performed preexercise and postexercise (1, 3, 5, 7, 10, and 15 min after the end of the exercise). A mean (± SD) interval of 6.2 ± 1.5 h (range, 4 to 10 h) between the methacholine and the exercise challenge tests was allowed in order to avoid any effect of the administration of the P2-mimetic agent on EIB evalua-tion.
An exercise test was performed on a bicycle ergometer while subjects were breathing dry medical air in order to assess the presence of EIB, as well as the VL (see below). The power output was increased during the first 4 min in order to reach a target ventilation output that was > 60% of the predicted maximum voluntary ventilation (35 X FEV1) according to standard recom-mendations. To ensure that the ventilatory stimulus for EIB was sufficient, the exercise duration was modified compared with recommendations to a total of 16 min (ie, 12 min at target ventilation). In addition, increased exercise duration may lead to bronchoconstriction during exercise itself, and we hypothesized that this bronchoconstriction may promote VL. Spirometry was performed preexercise and postexercise (1, 3, 5, 7, 10, and 15 min after the end of the exercise). A mean (± SD) interval of 6.2 ± 1.5 h (range, 4 to 10 h) between the methacholine and the exercise challenge tests was allowed in order to avoid any effect of the administration of the P2-mimetic agent on EIB evalua-tion.